Again, I was told to arrive with an empty stomach (no food or water after midnight) with a hospital bag in case we needed to go directly from the doctor’s office to prep for emergency surgery.
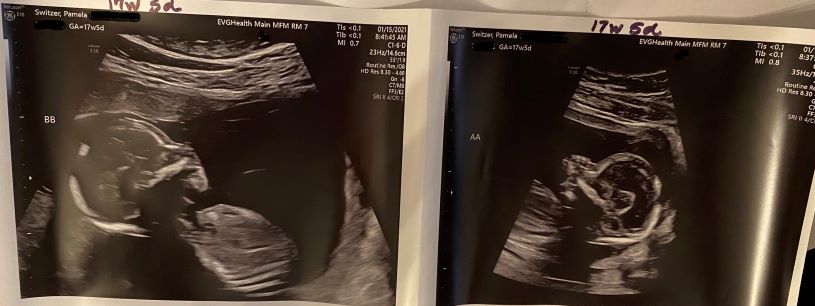
After a another comprehensive ultrasound with Doppler studies Dr. Paek came in to review the results. Fluids remained the same but the Doppler showed the blood flow in Baby A’s MCA had improved! We’re starting to understand no bad news is actually good news. We’re also beginning to understand that we will live ultrasound to ultrasound until these babies are delivered.
I’m scheduled to come back Monday Jan 18th.
For the record, Dr. Walker and Dr. Paek have been the most compassionate doctor’s I’ve ever seen. I had low expectations of bedside manner since they’re surgeons; I’ve come to expect through experience that surgeons know their field of expertise and compartmentalize the horrors they must endure. I don’t expect them to be kind or to be able to truly explain complicated medical conditions, symptoms and surgical techniques in layperson terms. These two people have treated me with more humanity and kindness that I ever expected while maintaining the utmost professionalism. This culture is prevalent from the nurses who check me in and ready me for grueling ultrasounds, to the techs who draw my blood, to the surgical coordinator Melissa who has been phenomenal to me since the day I was referred. I requested to fully transfer my OB care to this practice not only because it appears we will have a long road (not just a consult with resolution that might send me back to my Swedish MFM doctors) but also because the level of compassion and quality care I am receiving has literally blown me away.
I believe with my whole heart and soul that I could not be getting better medical care or in better hands. Thank you, God, for divine intervention when we need it most.
I was told to arrive with an empty stomach (no food or water after midnight) with a hospital bag in case we needed to go directly from the doctor’s office to prep for emergency surgery. I arrived tense and hoping for better news.
After a comprehensive ultrasound with Doppler studies (2.5 hrs) the specialist came in to go over the results. Everything about TTTS and related conditions is a study of blood flows, measured by the Doppler studies, and measurements – measurements of the babies to chart growth, measurements of the organs, measurements of the MVP fluid pockets, and measurements of the blood flows in and out of organs, the Medial Cerebral Artery (MCA), umbilical cords, and placenta. The amount of data our medical team must gather and review in order to understand were we are on that given day is staggering.
Today’s Diagnosis TTTS Stage0 with Expectant Management at this time
Our babies were borderline TTTS so since they didn’t meet the full criteria of Stage1, Dr. Walker called them Stage 0. In TTTS, one baby is large and called the recipient because that baby is getting more flow through the umbilical which causes many down stream symptoms like increase fluid around him and this increases pressures which result in stress on his organs and heart which lead to brain damage and heart failure. The smaller twin is called the donor because he is getting less supply through his umbilical, usually due to structural issues with his umbilical cord, poor umbilical cord attachment, and less placental share. These issues lead to symptoms such as too little amniotic fluid that further causes his bladder not to fill and disappear from ultrasound view, slow growth, and eventually Stage 5 which is death. One of our twins had too much fluid measuring MVP 9.6 (anything >8 is too much with 5 being normal) and our other twin measured at 3.9 MVP which was trending too little. For TTS Stage 1 the fluids must measure >8 and <2 – our babies are borderline and their bladders were both visible (TTTS Stage 2 when surgery is indicated is marked by the donor’s bladder disappearing). Their Dopplar studies showed elevated blood flows in small baby’s brain or MCA but not high enough to warrant surgery. To be clear, surgery isn’t advised until both babies are at lethal risk because surgery itself poses lethal risk. There is a 5% chance of spontaneous pregnancy termination from the invasive nature of the surgery. The placenta is very fragile and the vascular nature lends itself to rupturing when poked and prodded. The placenta is more mature and resilient at about 20 weeks, but becomes too mature and the vessels too large for surgery by 25-26 weeks. This window of approx. 4 weeks is really the surgery’s opportunity for the most successful outcomes. By successful, they mean cutting all vessels to Twin A so that when he dies, he doesn’t take Twin B with him. Surgery is targeted at preserving the life of one twin. Occasionally both twins survive, but usually a twin that has little placental share deteriorates and passes away after surgery.
When I asked what can I do? The only thing I can do is get more bloodflow to the uterus and take in nutrition. So. side-lying, horizontal rest begins now which increased bloodflow to the uterus and placenta, along with greatly increasing my nutrition to try to get more support to Joshua. My doctor has recommended I take in daily a minimum of 175g of protein and 2200-2500 healthy calories and 90 oz to 1 gal of water per day. That’s basically a diabetic diet with 3 additional 20-30g shakes (protein smoothies made with fresh fruits and greens) or Ensure Max 30g protein/4 g carb nutation drinks. Other than getting up for bio
In scouring the web for information on TTTS and TAPS, I found an amazing source of hope and heartbreak, and resources. The Twin to Twin Syndrome Foundation https://tttsfoundation.org/ . The found of this foundation experienced TTTS firsthand and lost her small twin Steven in 1989 because ultimately doctors at that time had little understanding the condition and no treatment options. Mary made a promise to Steven that he would be known and remembered and that she would find the answers. She has. Mary has connected mommas like me, bewildered by this “rare” diagnosis with the few specialists/surgeons who can treat it. She’s created support groups (using social media for good) for the newly diagnosed to help us manage our emotions, hear from the only other people who can truly understand this burden of fear and hope all mixed together, and the dynamic situation that forces us to be still and wait. This foundation has elevated awareness, resources, and success stories that bouy the spirits and raise the hopes of those of us who’ve already lost to the odd, the statistics that say “most mono/di pregnancies have no complications.” Statistics are of little comfort when they keep stealing your hope and forcing you into a smaller and smaller abyss. TTTS Foundation raises the battle cry to fight – fight with prayer, fight with hope, and fight with science. I cannot express how grateful I am for Mary and her promise kept. If you are looking for worthy nfp for donation this or any year, please consider one that helps save babies and supports women in their darkest hours.
The Details on our Diagnosis | further complicated
My Placenta
A healthy, typical placenta is anterior (located in the front of the uterus), posterior (the back of the uterus between the baby and mom’s spine), or fundal (on the top of the uterus). Most fetal surgeons won’t attempt a surgery on an anterior placenta for TTTS because it’s difficult to access from inside the uterus (think how does a laparoscopic laser instrument that is straight possibly curve 90 degrees to photo coagulate the inside of the front of the belly? Rarely will any fetal surgeon agree to attempt surgery on a mutli-sided placenta. I happen to have both – my placenta is anterior, fundal, and posterior with the area needed for surgical photo coagulation anterior.
Our Twins | Artery to Artery Anastomoses
Structurally, all mono/di twins share placental blood vessels and connections: they are truly sharing the same apartment living in different rooms. However, my twins have a large artery to artery anastomoses. This is essentially a large artery in Baby A’ s umbilical (my slammer baby) to large artery in Baby B’ s umbilical. This flow allows Baby A, my small twin, to garner nourishment from Baby B who is getting too much.
Our Twins | Doppler studies possible TAPS
Doppler studies are conducted on the blood flows in and out of all of the major organs, the umbilical, and placenta. Today’s Doppler indicated that the flow of blood through Baby A’s MCA was too high and might indicate early Twin Anemia Polycythemia Sequence TAPS.
Our Twins |Placental Share
At this time, Baby A has approx. 20-25% placental share while Baby B has 75-80%. The placenta continues to grow throughout pregnancy but is considered mature at 34 weeks so this very imbalanced placental share could improve or it could worsen. Should the small twin stop growing and deteriorate, this is an indication of placental insufficiency which is backward looking – we don’t know if the placental share he’s getting is insufficient to sustain his life. Based on his growth rate, it’s highly unlikely he would survive FLP.
Our Twins | Umbilical Cords and Cord Insertion
Baby B, our big baby, has a healthy 3 vessel umbilical cord with a secure connection to the placenta, and treelike vessels spawning into the placenta to give him adequate share of flows he needs. Baby A has a 2 vessel umbilical (less through put) along with a velamentous cord connection. This is when the umbilical cord abnormally connects more on the uterine wall along on the edge of the placenta along the chorioamniotic membranes, causing fetal blood vessels to travel unprotected from the placenta until they come together and reach the protection of the umbilical cord. Think of it as if you planted a plant on the rim of a flower pot; the roots would have to travel down the inside of the pot unprotected to make it to the soil for nutrients.
Current Treatment Path | Expectant Management
In a typical pregnancy the frequency is 4 weeks between ultrasounds until later in the pregnancy when it switches to 2 weeks. In mono/di twins the frequency is every 2 weeks. I’ll be monitored every 48-72 hours at this point. The goal of expectant management is for nothing to worsen, and to creep along toward viability which is 26 weeks or more gestation. We’re told to expect the longest our twins will gestate is 32 weeks. Expect that I will be hospitalized by 24 weeks, and expect preemies with long NICU stays. I’m incredibly fortunate to work for a company with values that support me caring for my family, allowing me to take leave and focus on this journey. I try to remind myself it is temporary, but the days are long and the weeks are longer.
During my 16 week ultrasound, I began to wonder what was actually happening. My ultrasound (which usually takes 2 hours, that’s right folks – one hour per baby) ran very long. The sonographer chat stopped. She left the room and came back several times, once bringing another sonographer with her to get an image she was having trouble getting. I hoped for the best but was on alert.
When I sat down with my perinatologist after my ultrasound and the conversation about my vitals, bloodwork, and pregnancy symptoms. It seemed like perhaps my suspicions were for nothing. Then she said, “ok, I need to talk for a few minutes.” She went on to tell me there were issues with the size difference or discordance of my babies. One was significantly larger, one significantly smaller and when the discordance is greater than 20, it’s abnormal. Mine were 25% discordant. Other concerns are umbilical connections and vessels in cords, the shape of the placenta, and maximum visual fluid pockets (MVP) Baby A 3.7 and Baby B 6.9 – all indicate early diagnosis of the dreaded Twin-to-twin Transfusion Syndrome (TTTS).
She said she needed to refer me to the nearest specialist and fetal surgeon for TTTS and related complications but they were already closed for the day. She’d call personally on Monday to ensure I got an appointment next week. He eyes were concerned, haunted. It was clear this is serious. I’m certain my heart stopped. Everything I had researched, everything that I had hoped would pass us by. We were headed to be in that 20% of mono/di pregnancies with complications. I couldn’t breathe. I made my way, in a kind of numb shock to the parking garage, swiped my card to pay for my parking, and found my way to the freeway.
As I pulled onto I-5 South for my 2 hour commute home alone at nearly 5pm (2 hours later than expected), I did what any self-respecting woman would do: I cried in my car. I sobbed like my heart had been broken in two.
They look so perfect, so healthy. How can this be?
We chose to announce broadly at Christmas because sometimes when you wish for a miracle, you do get two! Sam is almost 3 years old and has begun to speak in sentences. He’s learned about Santa this year, and learned his first Christmas carols. It’s been such a special season to sing with him, watch the Grinch for the first time, decorate our tree together, and hear his 3 year old musings about life. He’s going to be such an incredible big brother. So very special.
Yay! Santa’s coming and I’m going to be a big brother!
I’m already bumping. Fun Twin Pregnancy fact: a woman carrying twins is gestationally 8 weeks larger. So at 15 weeks pictured, I look 23 weeks along. This will get even more fun as the pregnancy progresses.
Thanksgiving Day: we’re truly thankful, grateful, and blessed to be expecting.
Sam is beginning to understand he’s going to be a big brother.
Our news brought great joy to our family members as we told them on Thanksgiving Day. The year has been wrought with terrible news in the US and abroad. News of not one but TWO babies to arrive in the summer of 2021 truly lifted spirits from coast to coast!
Identical in size and growing well. They’re perfect!
It was at my first regular appointment that I had my first sense of foreboding. Although we had discussed our plan for preeclampsia mitigation and transfer to Maternal Fetal Medicine who are all perinatologists, which is a fancy name for OBGYNs who specialize in high-risk pregnancy, I was unprepared for the anxiety I saw in the face of my OBGYN. This is the woman who admitted me to the hospital not once but twice on the verge of a stroke or heart attack. The first time at 31 weeks with severe preeclampsia that was untreated, completely ignored by my OBGYN at the time. Then she admitted me again directly from the NICO to the 5th floor with a preeclampsia flare up that sent my BP to 201/100 just a week after I delivered my son at 33 weeks. This is the doctor that saved my life twice. The look on her face was disconcerting. When I said, ” I thought our plan was to transfer me to MFM at the first sign of pregnancy induced hypertension (PIH) or HBP which would lead to preeclampsia?” She said, “our plan has changed: you’re carrying mono/di twins – we don’t even care for any mono/di twins in our practice, your history notwithstanding; we transfer them all immediately to MFM.” She went on to explain that while most mono/di pregnancies deliver near term with no complications, 20% have serious complications and she’d make sure I got the best care possible. I remember feeling confused and concerned when I left her office.
I went home and began researching like crazy. What I found on the internet was nothing short of harrowing. I copied urls and made notes. I read statistics that all seemed rather abysmal. I decided to be informed but prayed that my babies would be in the 80%. I readied myself with the facts.
What is the recommended timing for office visits for twin pregnancies?
Uncomplicated Twin Pregnancy Recommended Timing of Office Visits
TWIN CLASSIFICATION
STARTING AT
OFFICE VISIT
Dichorionic-Diamniotic (Di-Di)
First prenatal visit 28 weeks 36 weeks
Every four weeks Every two weeks Every week until delivery
Monochorionic-Diamniotic (Mo-Di)
First prenatal visit 16 weeks 36 weeks
Every four weeks Every two weeks Every week until delivery
More visits, more monitoring. We’ll just understand the risks and be ready at each visit with the proper questions.
Possible Complications
The scariest and most prevalent complication seemed to be Twin-to-Twin Transfusion Syndrome (TTTS). I read everything I could find by a reputable sources like Johns Hopkins and Children’s Hospitals across the US. There really isn’t a lot of information. From what I found there are only 8 or so fetal surgeons or specialists that treat TTTS in the entire US. Most people fly to get treatment. I was especially horrified to read that 5% of mono/di pregnancies are diagnosed with TTTS too far along for intervention resulting in fetal mortality. I learned that the earliest it can be diagnosed is 16 weeks and early intervention is the must successful. My plan is to be prepared with the proper questions when I go into each visit with my MFM perinatologist. I will not just “do what my doctor tells me to” like I did in my last pregnancy, when my concerns were ignored week after week while my BP rose untreated. That advice almost killed me and my baby. I’ll be vigilant and vocal this time. This time will be different.
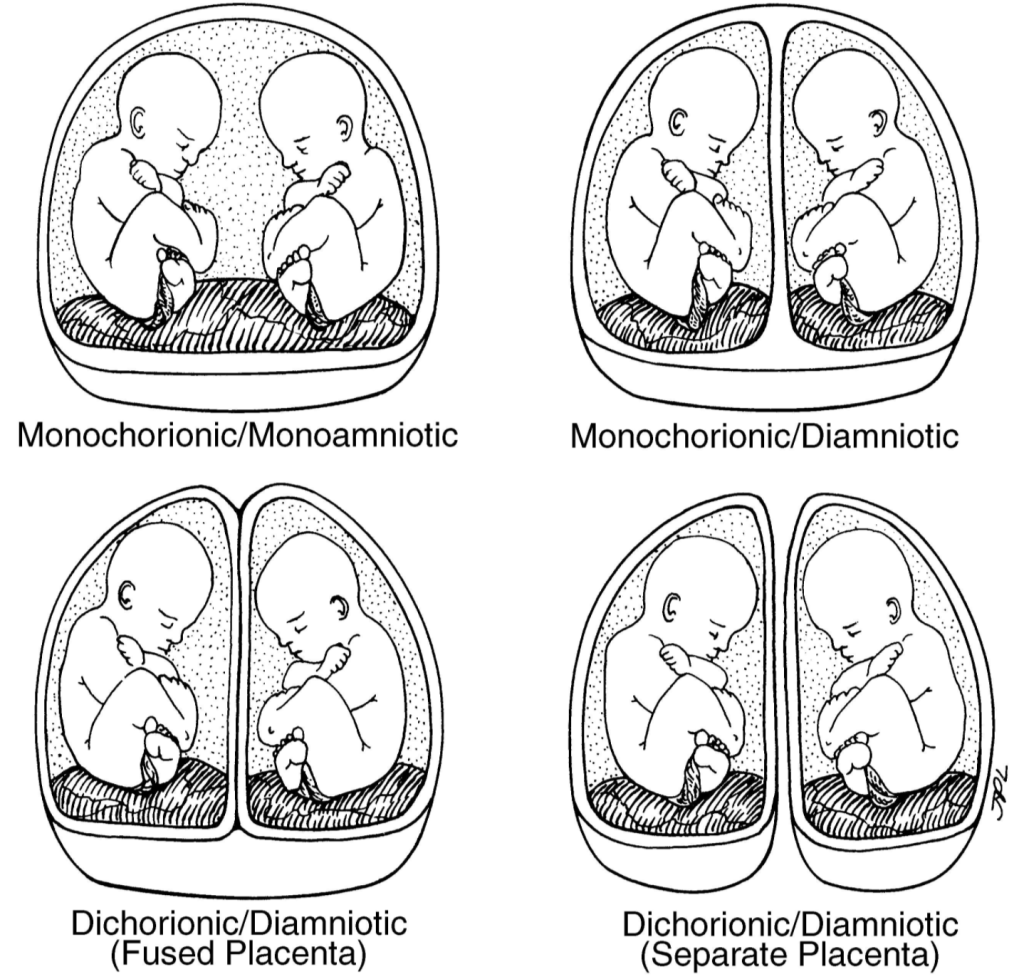
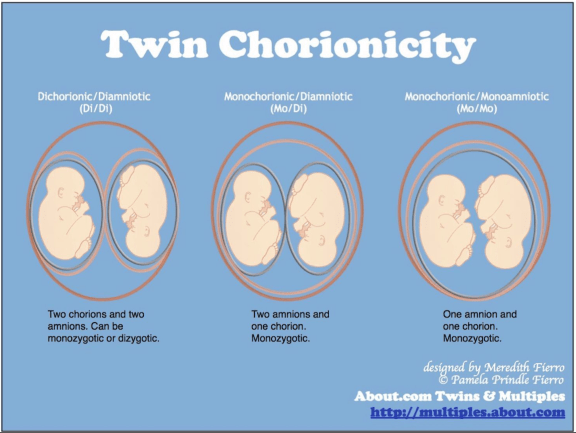
There are actually 4 types of twins. The type is determined by both the chorionicity (the outer membrane) and amnion (the inner membrane) and how the placenta is or is not shared. I found the best explanation at https://www.verywellfamily.com/twin-chorionicity-explained-4114659 . Visit that page for more.
“The terminology associated with a twin pregnancy can be confusing and overwhelming. Finding out that you’re having twins is just the beginning of an exciting experience. Along with adjusting to the idea of having two babies at once, there is a lot to learn. Here’s a guide to understanding these terms, and what they mean for the developing fetuses.
During a twin pregnancy, you may have heard the terms “Di/Di” or “Mo/Di” used to describe twins. These terms are used to classify and explain twin anatomy in the womb. Although it may sound like a lot of medical gobbledy-gook, they’re important concepts for parents because some twins are at risk for complications.
Let’s start by understanding the environment. In the womb, a fetus grows within its mother’s uterus. The placenta attaches to the wall of the uterus and serves the dual purpose of removing waste and providing nutrients to the fetus. It connects via the umbilical cord to the baby.
The fetus is enclosed in a fluid-filled sac surrounded by a thin membrane, called the amnion. A second membrane, called the chorion, surrounds the amniotic sac. Let’s break it down:
Mo: Means one
Di: Means two
Chorion: Is the outer membrane
Amnion: Is the inner membrane, which forms a sac filled with amniotic fluid containing the fetus”
What this means is that di/di twins or paternal twins and rarely have twin pregnancy complications because they each have their own placentas, amniotic sacs and chorions. Mono/mono twins are the most at-risk twin type and have a very low survival rate, because their umbilical cords tangle and terminate the pregnancy.
So for us, our twins are mono/di or identical twins, who developed from one embryo, that have the same outer membrane, separate amniotic sacs they share the same placenta and that is the root cause of most mono/di twin pregnancy complications. 80% of mono/di twins have rather normal gestations. That leaves 15-20% of mono/di twins who do experience complications.
At 5 weeks 3 days, it’s hard to see in still image, but when the sonographer rolled the ultrasound wand over the gestational sack, there are clearly two embryos now indicating the embryo split into two.
After calling to report having some bleeding accompanied with cramping overnight, SRM had me come it to determine if my pregnancy was at risk or had terminated. When the sonographer rolled the ultrasound wand and two embryos were clearly visible, all the air left my lungs. My eyes went wide in some biological response to make sure I was actually seeing what I thought I was seeing. I said, “is that what I…” She just looked at me for a moment and said, “would you be happy if there were twins instead of a singleton?” I may have just laughed a bit maniacally picturing Mark’s face when I had to tell him. I regretted not having FaceTimed the appointment. Mental note: FaceTime all appointments from here on out.
11/02/2020: SRM did their final ultrasound and graduated us as a confirmed pregnancy to the care of my OBGYN.
Like I shared during my two week wait, I began having the common pregnancy symptoms very early. However, since I’m undergoing assisted reproduction I take oral and injected hormones that cause the very same symptoms as pregnancy, I can’t really trust them to be an indicator of anything. In fact, assisted reproduction pregnancy symptoms aren’t as reliable in the first weeks and really up to the 12th week of pregnancy for those of us who could not conceive naturally. At 12 weeks, I will stop all oral and injectable hormones, the placenta takes over manufacturing those hormones, and I will then have more reliable symptoms that indicate what actually might be going on in the pregnancy.
Having said that, I feel terrible. Not like ‘over 40 and terrible’ because I’ve done that already. This is different. The nausea is far worse. The pressure in my uterus on my bladder THIS EARLY has me in the bathroom every hour to empty my bladder. The fatigue is extreme. My skin is becoming drier than a soup cracker. My hair is falling out. My sleeping is already interrupted by pregnancy induced Restless Leg Syndrome (RLS). I’m beginning to wonder what we were thinking. Can I really do this? Or is something off…. and so begins the worry.
Today’s blood test showed hormone levels increased from 300 on 10/12/2020 to >1000 today: pregnancy confirmed! We’re officially expecting our new arrival on June 20,2021!