Both of our babies experienced growth in the last two weeks. Baby B or Daniel is almost in the 80th percentile, and baby A , or Joshua has gone from fifth back up to the 10th percentile!!! Since we were told to expect it to continue to drop until delivery, baby A or Joshua’ s upward growth has delighted us!!!
The Caveat
Of course, there always seems to be a caveat! Mark rushed me to the hospital on Monday at noon, Because in my abdomen I was in excruciating pain. I was sure that we were in preterm labor and that we were losing our babies. Although I have had an increase in my cough caused from the pregnancy rhinitis over the weekend, I didn’t feel like I coughed any harder than in my last pregnancy. However with this pregnancy my belly is stretched so tight due to carrying enough amniotic fluid to support four pregnancies as well two entire babies makes me gestationaly bigger. All things being equal, a woman‘s uterus carrying twins at 23 weeks is physically equal in size to a woman carrying only a single baby at 31weeks. Perhaps being so stretched made my abdomen perfect for a tear, or perhaps it was something else I lifted or a combination of these- but I had ruptured my abdominus rectus muscle. It was bleeding into my abdomen, covering my entire right side of my baby belly from my ribs to pelvis in a huge hematoma. The pressure caused by the hematoma triggered contractions that could end my pregnancy and as a bonus felt like a wild animal with burning hot claws, searching for treasure inside me. My doctor came to the ER and helped get us the best care, which was ultimately able to stop the contractions and manage my pain. The plan is to get me healed enough to be able to take care of myself and then I can go back on bed rest at home maybe by Friday or Saturday. However the critical weeks are ahead – weeks 24 through 28 during which, if the babies show more signs of distress we would return to hospital and be on antepartum care in the hospital until they’re born.
i am extremely grateful for the excellent news on our babies this week. I’m also grateful for the perspective that a torn muscle can give me. If the babies are OK, then we’re all OK!
Tuesday’s appointment went better than expected: the twins’ numbers were essentially unchanged. Their fluids improved slightly with Baby A holding at MVP approx. 7 and Baby B had a little less fluid at MvP approx. 12.5 which is very good trending for fluids. Our doctor said these numbers may be a signal that they’re stabilizing! Dr. Walker was even positive about their cardiology report: he said Josh’s heart defects were diagnosed better than he thought and Daniel’s would likely resolve before birth. We’ll keep tracking their hearts and be prepared for what might come next after they deliver. The priority is keeping them in utero as long as possible, getting them ready for life outside the womb.
Next Tuesday 2/23/21 their growth is again measured, and we’ll see if Joshua’s (Baby A) percentile improves. Our doctor emphasized that weeks 23-26 are critical; if they go well, we may be able to keep them in longer to like 30-32 weeks. If not, they become viable for delivery as ultra preemies at 26 weeks. Your prayers and healing vibes you’re sending our way are everything: keep up the positivity! Thank you so very much for your words of encouragement.
Approx. 22 weeks, they’re eyes are fully formed but their eyelids are closed, they have hair now along with eyelashes and eyebrows, and are beginning to hear sounds. They’re wrinkly now until they gain body fat to add the padding that plumps them into chubby babies ready for the outside world. Technically, they’ll be viable in 4 more weeks if both are >500 grams in weight.
Snow socks are in; chains are so last year! Apparently, my vehicle doesn’t have enough clearance for chains (this is the future of new vehicles) and this nifty new accessory called “snow socks” provide the same traction as chains but like 1% of the hassle! I slid them on the top half of the tires, rolled my swagger wagon forward, then slid the other side on – just like a sock. These socks got me up several icy hills and across an iced overpass in the dark on the way to hospital. My new favorite car accessory. The hospital maintenance people watched in awe as the hugely pregnancy woman did the reverse process in the parking garage in under 4 minutes after my morning appointment. Because like chains, these have a max speed of 30 mph which is a no-go for the freeway which was clear by the afternoon.
Today’s Summary | No surgery equals a win
After staying overnight in a hotel .25 miles from the hospital to make sure I could get there no matter how much snowfall we received overnight, my 2.5 hours + of ultrasound and Doppler studies showed that everything remained approximately the same, so in short – no surgery today! Hoorayyy! We’re making peace with the reality that no action is good, no worsening news is great news, and the longer we can put off any procedures of any kind of poking or surgically going into the womb is a win. “No action” is not intuitive nor does it feel right: never before in our lives when facing a problem has doing nothing made sense. Yet, every day that we do nothing, we cross off the calendar as a win on on our march toward healthy viability (April 1) because it is a success. Onward we march. Of course, I fully believe that my doing the recommended, as much side-lying horizontal rest and forcing nutrition (it’s actually not very easy to take in 175 g of protein per day and 90 oz of water) along with the support sent by prayers and positive energy coming from you, our tribe of supporters, is making all the difference! Thank you for keeping up the goodness: this is a temporary situation which will all be over before summer, ideally between April 24 – May 09 (if by some incredible stroke of luck and miracle of modern medicine we could keep them in until 32-34 weeks).
More details from today’s Surgical Team/MFM visit
Amniotic fluid is measured via Maximum Vertical Pockets (MVP) which have a small +/- because the uterus isn’t a fixed shape like a sphere. Each time they measure, the uterus shape is slightly different and the measurement is taken by finding the deepest area in a vertical line, without the baby or any of his parts in the line. So the measurement varies a bit day-to-day by nature of the shape. Today, it was approx. 6-7 cm for our smaller baby, Joshua and approx. 13.5-14.5 cm for our larger baby, Daniel. Total fluid remains at about 20 cm which is right on the line for causing contractions and cervical failure which leads to premature labor.
Doppler flows measured approx. the same, too.
Cervical length (which is discussed because it is the determining factor in all of the above) measured a bit better after two days of almost complete side-lying horizontal rest at approx. 3 cm up from 2.5 which is nearing the shortness that requires cerclage due to it basically failing to hold under the weight of all that fluid plus the babies.
Their Hearts | diagnosis from Seattle Children’s Hospital Cardiology
Our MFM team found some abnormalities with Baby A’s hearts, referring us to Seattle Children’s pediatric cardiology. After another 2.5 or so hours of ultrasound echo cardio + Dopplers focusing on the babies hearts, we found out that both of our babies have a relatively common heart defect right now. The “good” news is that these defects do not really affect the growth of the babies while they are in utero, cannot be treated in utero, and if they are still present at birth, the babies will either need no treatment, surgery within 3-6 months of life, or surgery immediately after birth for which they would be transported by ambulance to Seattle’s children and then would recover in Seattle Children’s cardio NICU. Honestly, with all we have going on, this problem is the least of our worries right now. That’s really saying something when open heart surgery of your preemie newborn(s) is the least of your worries. We’re putting off worry about this: we’ll cross this bridge when we come to it.
More details from today’s cardiology visit on hearts
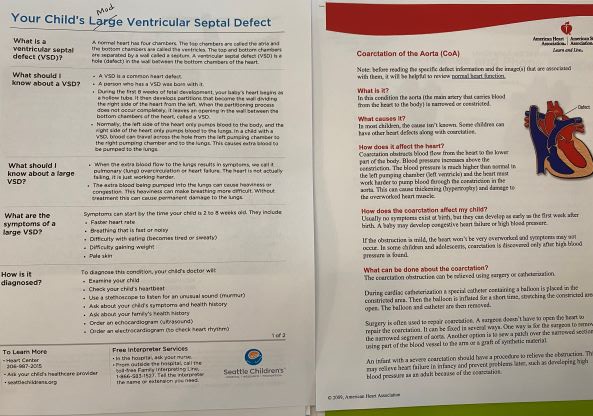
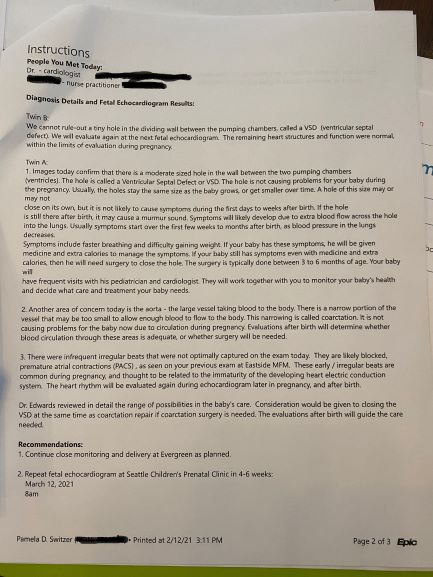
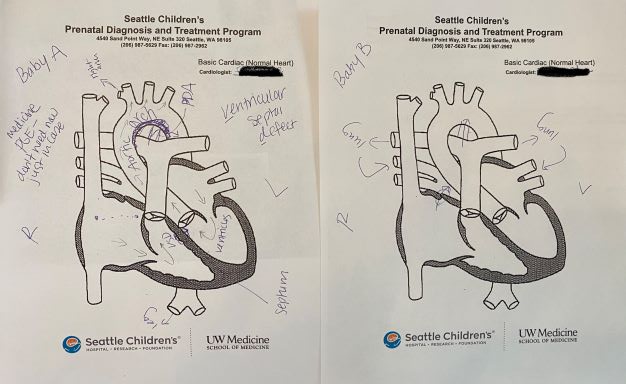
Baby A has two relatively common heart defects. Both Baby A and B have a small hole in the septum between their left and right ventricles (the part of the hear that squeezes to push the blood through. These holes are called Ventricle Septum Defects VSDs. 1% of all pregnancies have this defect and in some babies, the hole repairs by closing on its own before birth. The location of Baby B’s indicates his might close on its own, but the location of Baby A’s makes it a lot less likely that it will close on its own before birth. Baby A also has a narrow aortic arch or a Coarctation of the Aorta (CoA) assessed as Moderate (not quite mild and not severe). If both of these issues are still present in Baby A at birth, he’ll likely need open heart surgery the day or few days after he’s born. We, of course, are praying this all resolves with growth and time in utero. One thing is for sure, their hearts aren’t the only heart with a hole in it until they’re born…
The PDA is a fetal vessel that acts as a temporary bypass which allows blood to push to the body if the aortic arch is too thin during pregnancy. This PDA vessel begins closing at birth which is why the heart surgery to correct a thin aortic arch or (CoA) is done after birth.
Thank you all. Remember to play and fill your hearts.
Today was a day of small miracles. So, it goes in the win column. I was able to get home before the snow began to fall in earnest, rather than being snowed in at a hotel 50 miles away from everything that matters to me in this world. Thank you to every single person reading my updates and reaching out to make sure I don’t feel alone. Your cards, notes, texts, and words of kindness (large and small) are helping me find my ‘eye of the storm’ zen every day. You’re all keeping me sane. I hope you’re filling your own tank during this isolating time: I hope you’re daily finding moments of joy, reminding yourselves to play, and if you’re in the PACNW maybe making a snowman today.
Watching my son and his daddy snowsled today, hearing their laughter, and seeing my dogs (even my 12 year old senior) romp like pups in the deep snow reminds me of what truly matters in life – the small everyday moments are the stuff of dreams.
Pregnancy Threatened – preparing for a decision to treat Polyhydramnios on Friday 2/12 7:30 am…with record snowfall predicted to begin Thursday afternoon.
The Details
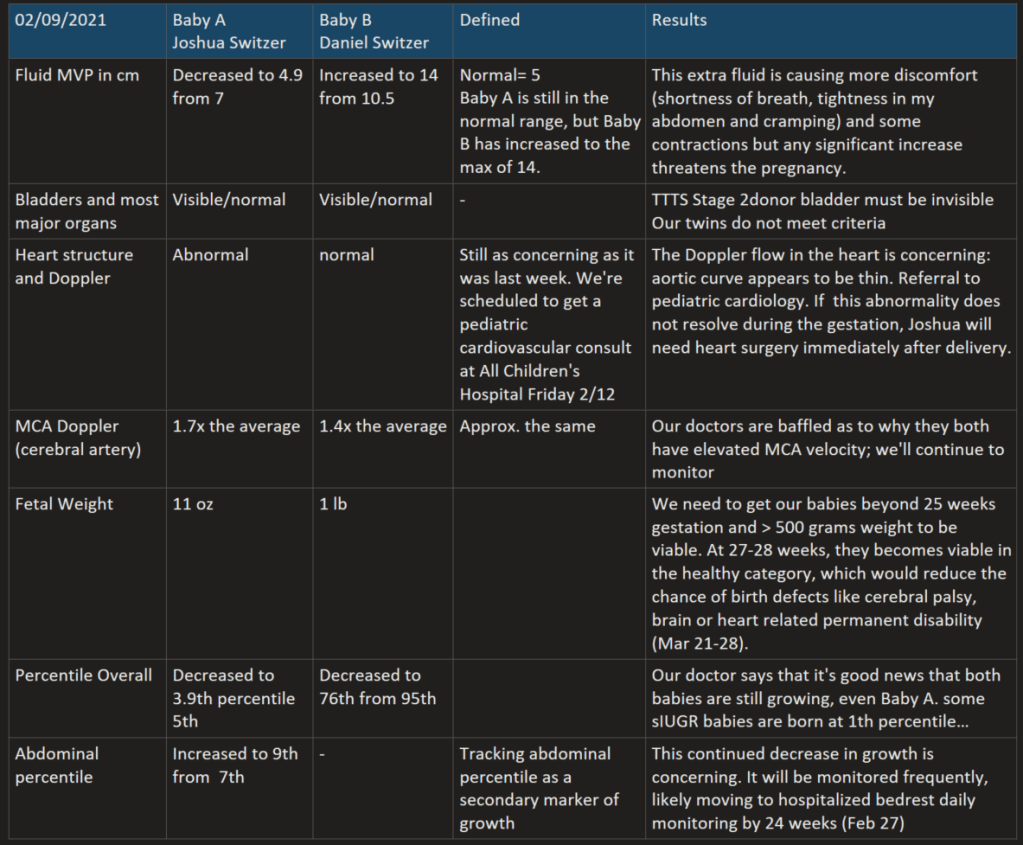
We had hoped for good news today but instead, we received more jarring news. Both babies’ Doppler studies indicate they both still have elevated blood flow rates in their cerebral arteries, which is usually indicative of anemia. But, they both aren’t showing any other signs of anemia so we’re going to continue to monitor this symptom to see if it leads somewhere. The growth numbers decreased in both babies: our large baby dropped from 95th percentile to 76 and our small baby decreased from 5th down to just under 4th. Our doctor says that it’s good news that they are both still growing and gave us some new goals. We need to get both babies beyond 25 weeks gestation and > 500 grams weight to be viable. At 27-28 weeks, they becomes viable in the healthy category, which would reduce the chance of birth defects like cerebral palsy, brain or heart related permanent disability. If we can get them to March 21 or out to March 28, delivery would be a better option than anything else should Baby A’s growth stop.
The most immediate concern is to manage the condition that could cause loss of pregnancy. Polyhydramnios is excessive accumulation of amniotic fluid surrounding a baby in utero. It threatens the pregnancy in many ways – premature labor, placental abruption, umbilical cord prolapse, and more. My cervix is finally showing signs of too much pressure/weight from the fluid as well, so any option to treat includes surgical suturing of the cervix to keep it from opening (cerclage) which will be removed at delivery. Right now the larger twin doesn’t seem to be suffering any expected negative effects from this excess fluid, but if it increases again, he will. I return this Friday to have my fluids measured again. We were told that if the amniotic fluid around Baby B increases, we must be prepared to make a decision to treat it.
Option 1 is to reduce the fluid by draining the excess amniotic fluid with a large needle (amniocentesis).
Pros: 1% chance of the procedure causing loss of pregnancy (spontaneous miscarriage).
Cons: This does not address the underlying or root cause of the excess fluid, so it will continue to build up again and need to be removed again. We can continue to drain the fluid with the same procedure repeatedly until we can deliver but choosing this path means we no longer have the option to do Fetoscopic laser photocoagulation (FLP) at any time.
Option 2 is to do FLP where our surgeon uses a laser to block the blood vessels that communicate between the twins. This newer method of managing sIUGR ensures that the connecting blood vessels do not cause harm to the normal twin, while allowing the smaller twin to continue at its rate of development.
Pros: It can address the underlying cause of the polyhydrops, preventing excess of fluid for the remainder of the pregnancy. It also allows the smaller twin a chance at continuing development. Additionally, this preserves our larger twin’s life, if our smaller twin doesn’t survive over the next 5-6 weeks.
Cons: 5% chance of the procedure itself causing loss of pregnancy/spontaneous miscarriage. Since the procedure seals off the blood flow between the twins that may be keeping the small twin alive, cutting off his access could result in fetal death if his placental share is not enough to sustain him. The only way to know if his placental share is enough is in hindsight; there’s no way to know before we do the procedure.
It’s likely whatever procedure we choose on Friday will override my appointment at All Children’s Hospital so we’ll have to reschedule the cardio consult. Oh, and the snowstorm, because hey, why not!?! Since I live 50 miles from the hospital, I’ve booked a hotel room less than a quarter mile from the hospital where the streets leading to the hospital should be cleared/plowed rather early in the morning so that I can drive to my appt. If the snow is impassable, I could likely walk to the hospital on Thursday morning (as long as I give myself plenty of time to waddle up the hill – lol). In all seriousness, most women dealing with TTTS or sIUGR have to do this drill by flying to Los Angeles, Cincinnati or Miami. We truly are fortunate to have one of the top surgeons for this particular “rare” complication in the same state, even during a snowstorm.
Thank You for Your Support
Thank you again for all of your support, sending healing and prayers our way. Many people have a visceral reaction to the word prayer, or any word used other than prayer. Here’s why I use the words I am using in this blog (and in real life). As a woman who studied the Christian Bible for almost half a decade in preparation to go to seminary and later studied at a theological university, I value people, and these people often hold diverse beliefs and come from diverse backgrounds. The most distilled statement I can craft is that I believe the most important command of my faith is to value others and find unity rather than division (I’d be happy to have a deep theological discussion offline about where I find the doctrine and scripture to support, but I will not digress here). More simply put, I treasure people: I have friends whose beliefs are Lakota, Jewish, Hindu, and many different denominations of Christian that they may as well be different religions. I also value my agnostic and atheist friends. I find science and faith in harmony not odds. The science, psychology and metaphysics of prayer is becoming well documented. A decade ago, Psychology Today cited just a few studies in an article that shared this:
“An interesting bit of science attached to this ethnocentric and geocentric evolution of prayer comes out of Duke University Medical Center, where a study found that, within a group of 150 cardiac patients who received alternative post-operative therapy treatment, the sub-group who also received intercessory prayer (they were prayed for) had the highest success rate within the entire cohort. The fascinating thing about the study is that it was double-blind – neither the researchers, nor those on the receiving end of the intercessory prayer knew that these patients were being prayed for — suggesting an intervening variable.” <https://www.psychologytoday.com/us/blog/enlightened-living/201007/the-science-psychology-and-metaphysics-prayer>
I’m sure there’s more studies and evidence out there for those interested in doing their own due diligence. My bottom line is this: we are all connected. When a human being sends out positive intent, healing light and love, blessings, or prayer, the metaphysical reciprocal resonance that has been demonstrated to exist between states of consciousness – specifically, casual states of consciousness (prayer, meditation and deep, dreamless sleep) — and the quantum field (what we like to call reality) described by quantum physics. As a treasured friend of mine once said, “if you’re not paying attention to metaphysics, then you’re just not paying attention.” So, whether you hang your hat on science or prayer, both or somewhere in between, I value you and I desperately need you to send whatever positive energy you can toward my unborn sons.
Another heart felt thank you to everyone following our journey. May it end in April or May with a big celebration.
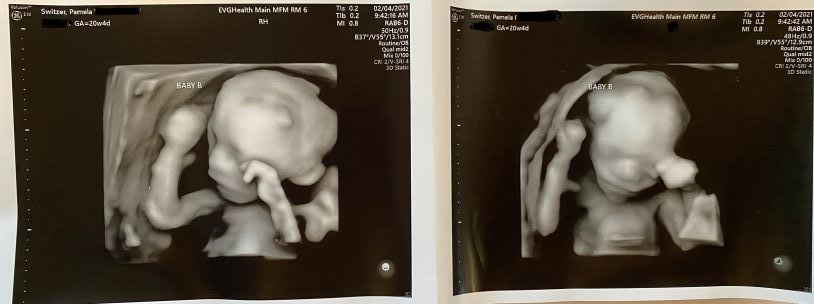
My sonographer did a neat 3D imaging on my boys. The lumps that appear on the imaging are caused by movement but the babies do not actually have those lumps. It is wonderful to see because it means they’re feeling well. Sick babies are lethargic in the womb.
Life until March 13, 2021 (26 weeks) is now lived scan to scan.
Today, the scans showed babies with beating hearts and lots of movement. Their fluids remain similar and their MCA Dopplers improved. Joshua’s (Baby A) reduced to around 1.5x AVG and Daniel’s (Baby B) has returned to normal. Our MFM perinatology and fetal surgeon team has admitted that they are somewhat baffled at the array of symptoms the Switzer twins are displaying which do not identify with any known constellation of symptoms indicative of a specific complication. Time and development will further refine our diagnosis. Our babies are not safe until they are delivered – they begin to become viable at 26 weeks on March 13th. Dr. Walker has adjusted my target delivery date to no later than 32 weeks on April 24 if we are fortunate enough to make it that far.
While our babies have some characteristics of TAPs, they definitely have sIUGR with artery to artery anastomosis. Friday 2/15 we’ll see a pediatric cardiologist to find out if Joshua has a problem with his heart that will require surgery at birth, or perhaps he’s just behind in growth. It’s clear that these symptoms and stats can change in 24-48 hours, but aren’t likely (no guarantees, of course) to change dramatically in under a week until I’m farther along. So, we continue expectant management on a weekly frequency unless something dictates a change to more frequent 2-3 times per week monitoring (which has happened 3 out of the last 6 weeks). At 24 weeks gestation (by the week of Feb 22, 2021) or sooner I’m to be admitted to hospitalized bed rest to have daily monitoring and daily access to emergency surgery. Until then, all I can do is maintain side-lying horizontal rest to increase bloodflow to the uterus and placenta and 175g protein/2500 healthy calories per day to boost nutrition, all in an effort to get more nutrition to Joshua.
The next growth scan is currently scheduled for Tuesday Feb 9, 2021. So, we hope, we pray, and we wait.
Thank you for your prayers, sending light and love, for injecting positivity and healing into the metaphysical connected consciousness for us. This means more to us thank you can possibly know.
How do we prepare for a surgical decision on Thursday?
What is selective intrauterine growth restriction?
Monochorionic twins are twins that share a single placenta. Selective intrauterine growth restriction (sIUGR) occurs when there is unequal placental sharing which leads to suboptimal growth of one twin. In cases of sIUGR, the estimated fetal weight of the smaller, growth-restricted twin usually falls below the 10th percentile. This will usually result in more than a 25 percent weight difference between the twins.
sIUGR is estimated to occur in approximately 10 percent of monochorionic twin pregnancies. There are three types of sIUGR that are determined by the blood flow pattern in the umbilical artery of the growth-restricted twin.
Review of sIUGR Type 3 (our diagnosis)
Unpredictable pattern of intermittent blood flow in the umbilical artery of the growth-restricted twin (forward, absent or reversal). In other words, only occasionally is the blood flow in the artery absent or flowing in a reverse direction. This type of blood-flow pattern is unique to monochorionic twins with sIUGR. It occurs when large arterio-arterial connections are present, allowing shared blood to flow back and forth between the twins.
Average age at delivery is 30 weeks gestation
In up to 15 percent of cases, the growth-restricted twin may not survive, which can also impact the neurodevelopment of the normally growing twin.
Whether or not the condition will change or worsen during pregnancy is difficult to predict from the ultrasound images. Babies with type 3 sIUGR are born, on average, during the 30th to 32nd week of pregnancy. Their overall survival rate is 80 percent.
Selective cord occlusion: This procedure may be offered if you have monochorionic twins with Type 2 or Type 3 sIUGR. Selective cord occlusion is a minimally invasive procedure that stops blood flow to the growth-restricted twin. The goal is to optimize the outcome for the normally growing twin. The procedure can be performed using bipolar cord coagulation, interstitial laser, or microwave ablation. Fetoscopic laser photocoagulation: In select cases this minimally invasive surgery can be used to laser ablate (seal) blood vessels that are shared between the babies. Similar to selective cord occlusion, the goal of therapy is to optimize the outcome for the normally growing twin. Delivery: If sIUGR is discovered later in the pregnancy or the condition progresses after the pregnancy reaches its 24th to 26th week, delivery of the babies may be the best option. How is selective intrauterine growth restriction (sIUGR) treated after birth? Most babies with sIUGR are born prematurely, but our goal will be to prolong your pregnancy for as long as possible.
I’ll say again, these words are so sterile and clinical but they mean choosing a car seat and a casket, or two caskets. In real life, these words are heart rending to the woman carrying these babies, seeing them on ultrasound with all of their fingers and toes, ears and lips, fully formed, approx. 10 inches long, occasionally sucking their thumbs or touching each other. They are already little people. They are my babies and I want to hold them, see them grow, hear them giggle, kiss their owies and hear them say “all better.”
The most painful of research
Instead, I’m researching the rules and regulations of burying stillborn babies. Some people will ask why I’m even looking at this information now. It is fact that I will deliver my twins on the same day. What is unknown is whether they both will be alive, stillborn, or one in each condition. I certainly do not want to go into my appointment on Thursday, have emergency surgery, and then have to give final resting instructions with no information, under duress and likely the influence of medications. So, I am researching.
In addition, I’ve chosen to name them because they need names. If we bury them, they need a service, caskets, headstones, and a gravesite. If we cremate, they need urns and other arrangements. I’ve learned that state law dictates how remains are handled. In most states after 24 weeks gestation, they must be buried or cremated. I am horrified at the thought that these tiny, perfectly formed little babies could be treated any differently at 20, 21, 22, 23 weeks. Certainly, at 20 weeks remains of fully formed babies are not medical waste to be burned in some hospital incinerator – not my babies. This is what people facing this horrible set of complications of mono/di twins do. They do their best to prepare for the unthinkable.
No gifts, no registry – we’ll wait until they’re delivered
Why? Let me explain. Last month, I received adorable baby gifts from a treasured family member. I dragged my feet for days opening the package. While they are adorable, and I called and expressed my thanks, it was bittersweet to touch these tiny onsies, wraps, and hats. I dragged my feet for another week or so deciding if I should cut the tags off and launder them to be ready for babies to come home from a hospital or not. I finally decided I couldn’t bear shipping them back, should bad or worse happen. So, I cut off the tags, feeling rather numb, laundered them, folded them and put them in a clean storage container sitting in my room awaiting the nursery to be put together. Since 1/26 when our sIUGR diagnosis began to worsen according to the data, I lose the ability to breathe every time I walk by it. I think, “what would I do if we had car seats and a pule of gifts we had to return?” Make my husband lug our dead babies’ car seats and boxes to UPS? It would be unbearable on top of unbearable. So it’s decided. No gifts, the registry is on hold. We’ll worry about clothes, gifts, and car seats after they’re delivered when we know for sure what is needed.
How do we manage from here?
Life has taken on a surreal duality: half of it is on hold and half must go on. Daily tasks feel like they betray the severity of our situation, but tasks like grocery shopping, ongoing reno decisions, bringing in the mail, paying bills, etc all must go on. Having acknowledged that, half my heart is on hold until Josh and Daniel get here. There simply is no peace until they arrive, God willing, between 26 (mid-March) and 32 weeks (April 24, 2021).
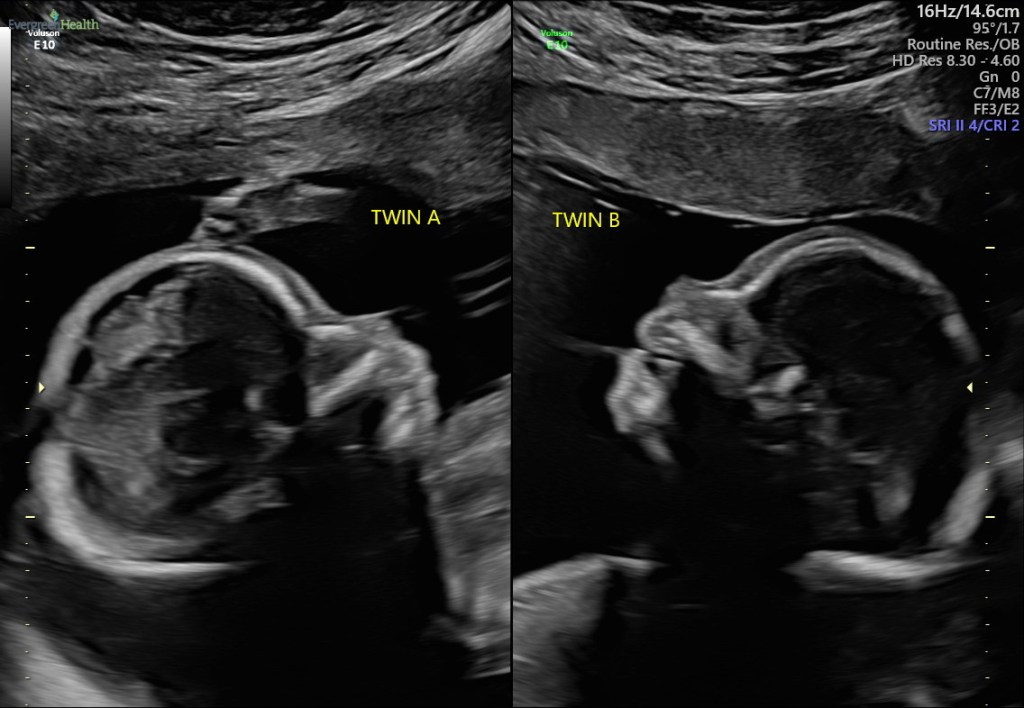
Baby A – Joshua on the left and Baby B – Daniel on the right at 20w1d.
Doppler crisis (again) + a new heart abnormality
After a weekend of contractions overnight all night on Saturday (which is highly unusual because the recommendation for stopping early contractions is hydrate and lie down with feet elevated) along with abdominal cramping, my medical team brought me in a day before my scheduled appointment.
While the fluid levels have improved, it feels like Baby A (Joshua) is deteriorating. He now has a problem with his heart along with his growth continuing to decline. Both babies now have abnormal MCA Dopplers in their Cerebral Arteries. I’ll come back in 48 hours on an empty stomach in case we have to do the dreaded surgery that might end Joshua’s life and potentially also Daniel’s. It’s our darkest hour thus far.
The goal is delivery after they’re viable – we’re at least 6 weeks away.
All the other options feel agonizing. The only thing that can be done is …wait. Come back in 48 hours. Life is just living scan-to-scan. Today it feels untenable.
The answer is random. Purely random. My surgeons have reiterated on almost every visit that there is nothing genetic or environmental – nothing I did, nothing in my genetics or Mark’s genetics, nothing we ate, breathed, or were exposed to – absolutely nothing we did to cause these complications. There are no indicators on who will and who will not fall into that 20% of mono/di pregnancies percentile that experiences complications. If we want to place blame, the only logical place is on the placenta at conception. At conception, the vessels and tissue that would become the placenta began growing and these issues all come from a placenta that wasn’t divided equally to each twin and grew abnormally. It does help me to hear this. It helps because I can see it in the eyes of others and hear it in their tone, the unwritten “well this is what happens when older women try to have babies.” My surgeons say that’s just not true or accurate.
The exact cause of TTTS is not fully understood. However, it is known that abnormalities during division of the mother’s egg after it has been fertilized lead to the placental abnormalities that can ultimately result in twin-twin transfusion syndrome. – National Organization of Rare Disorders
To be painfully honest, I wish I’d had a life where I grew up in one home rather than attending at least 14 different schools K-12. I wish I’d had a stable nuclear family and life, gone to college as a teenager, sorted out what I wanted to do and what I could do and began my adulting fully functional. I’ll spare everyone the details, but in short my life didn’t go that way. I managed with the cards I was dealt through some very rough patches from the time I left home at age 16 through my 20s and 30s. I finally found balance in my faith and science, a path to a post-secondary education, and the love of my life rather late in life. My only options were becoming a mom over age 40 or never becoming a mom. i chose to fight the limits of reproductive biology with science becoming a mom in January 2019. As much as I wanted to be a mommy, I was wholly unprepared for the expansion of love, compassion, and critical thinking motherhood would bring. I was arrested by the joy of watching my baby become a toddler with his own personality, thoughts, and dreams. Parenthood has made me a better person, the very best revision of myself because it isn’t about me. Parenthood is an immersion in investing in others. I am thrilled to be able to provide my child with so much that I never had and desperately wanted. I cannot wait to see who he becomes with solid resources and parents who are both interested and fully committed to him. If we’re lucky, just one more time, he’ll also become a big brother and the Switzer boys (Samuel, Joshua, and Daniel) will have each other long after their mom and dad depart from this earth. And maybe just maybe, they’ll contribute to our world becoming a better place. It is all of this that I hold in my heart and pray for every day.
Aren’t twins more common with fertility treatments? Isn’t the fertility treatment to blame? Aren’t older women more likely to conceive twins?
In a word, maybe. The data just isn’t clear In fact, the data is rather muddled because the data about twins doesn’t parse easily to explicitly show trends in fraternal twins (where two separate eggs fertilized) separate from identical twins (where one egg/zygote divides to create a multiple pregnancy resulting in twins, triplets, or quads). Until recently, fertility treatments for women over age 35 was to transfer multiple eggs in hopes one would result in a confirmed pregnancy. This technique proved to be false: my fertility specialist explained that conception is largely binary. Two embryos transferred results in paternal twins 70%, and since twin pregnancies come with higher risk and women >35 and especially >40 are already a higher risk group, fertility specialist no longer recommend or support multiple embryo transfers.
According to data collected by the Centers for Disease Control, there were 133,155 twins born in the United States in 2015. That’s 33.5 per 1,000 live births, or put another way, about 3.35% of live births. There were 3,871 triplet births, 228 quadruplet births, and 24 quintuplet or higher order births. These numbers include naturally occurring multiples, along with those conceived with fertility treatment. The overall rate of multiple births increased and peaked during the 1990s but has been declining over the past decade. The percentage of triplet and higher order pregnancies has dropped 36% since 2004.
In the general population, identical twin pregnancies occur 0.45% of the time, or 1 in 250 births. While most multiple pregnancies conceived with fertility treatments are fraternal twins, the use of fertility treatment does increase your risk of having identical twins.
According to one study, identical twins made up 0.95% of the pregnancies conceived with treatment.11 That’s double the general population’s risk. It’s unclear why fertility treatment leads to more identical twins. One theory is that the culture embryos are placed in during IVF increases the risk of identical twinning. Another theory is that treatments using gonadotropins lead to the increased risk of identical twins.
Following more than three decades of increases, the twin birth rate declined 4% during 2014–2018, to the lowest rate in more than a decade, 32.6 twins per 1,000 total births in 2018.
The number of births in twin deliveries declined an average of 2% per year from 2014 through 2018, dropping to 123,536 births in 2018.
Twin birth rates declined among mothers aged 30 and over, with the largest declines among older mothers aged 40 and over.
The twinning rate dropped 7% among non-Hispanic white mothers from 2014 to 2018 (34.3 in 2018), but was essentially unchanged among non-Hispanic black (40.5) and Hispanic (24.4) mothers.
Twin birth rates declined in 17 states and rose in three states.
So how can you tell if mono/di twins are on the increase or decrease if fertility treatments in the last 5-10 years went from predominantly multiple embryos transferred to single? The answer I hear from the front line is you simply can’t.
I leave you with the final Twin Fact: The U.S. twin birth rate declined 4% from 2014 to 2018. Twin birth rates declined by 10% or more for mothers in all age groups 30 and over.
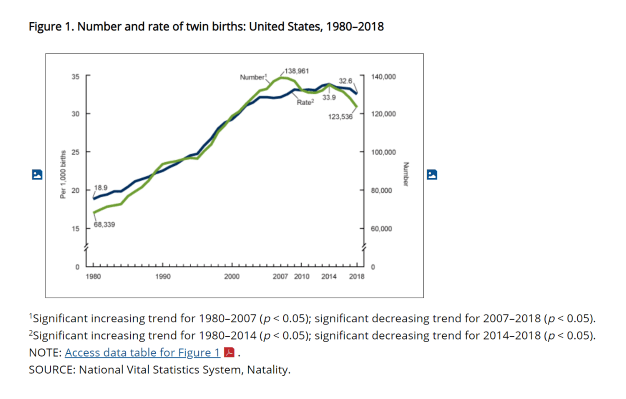
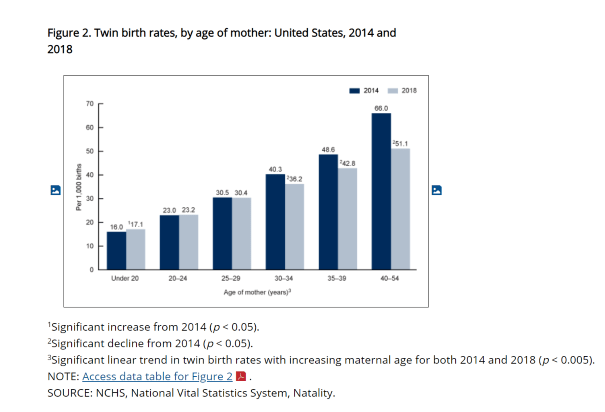
The twin birth rate rose by an average of 2% annually from 1980 (18.9 twins per 1,000 total births) through 2003 (31.5), for a total increase of 67%. The pace of increase then slowed to less than 1% annually from 2003 through 2014 (33.9) (Figure 1).
The twin birth rate declined by an average of 1% a year from 2014 (33.9) through 2018 (32.6) for a total decrease of 4%.
The number of twin births more than doubled from 1980 (68,339) to the peak in 2007 (138,961), then fluctuated from 2007 to 2014 (135,336).
The number of twins declined by an average of 2% a year from 2014 through 2018, to 123,536 twins in 2018, the lowest number reported since 2002.
The data doesn’t support that age is to blame as twin birthrates fall in all age groups 30 and over.
Twin birth rates declined for mothers in all age groups 30 and over; the rate fell by 10% for women aged 30–34 (from 40.3 per 1,000 total births to 36.2), 12% for women aged 35–39 (from 48.6 to 42.8) and 23% for women aged 40 and over (from 66.0 to 51.1) (Figure 2).
Twin birth rates were essentially the same between 2014 and 2018 among women in their twenties (from 23.0 to 23.2 for women aged 20–24, and from 30.5 to 30.4 for women aged 25–29), but increased for mothers under age 20, from 16.0 to 17.1.
In 2018 as in 2014, twinning rates increased with advancing maternal age. For both years, mothers aged 30–39 were more than twice as likely, and mothers aged 40 and over were three times as likely to have a twin birth, compared with their counterparts under age 20.
Mark and I have agreed we’ll each name a twin. Baby A’s name is Joshua and Baby B’s name is in flux but we’re calling him Daniel at this time. We’ll see if Mark changes his name by the time we meet him in-person.
This week’s scan stats.
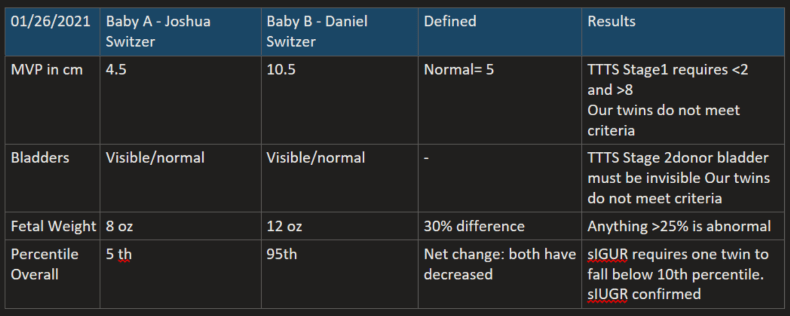
With normalized Dopplers, this week the TAPS diagnosis is put on the back burner along with TTTS. However, sIUGR is confirmed because Baby A’s growth falls below the 10th percentile, the diagnosis of Selective Intrauterine Growth Restriction (sIUGR) is confirmed. While sIUGR and our babies have Type 3.
Our treatment path is currently Expectant Management. As we do weekly or more frequent monitoring, conditions may change. Because the artery to artery flows between the babies are likely keeping Baby A alive, we will not consider surgery, because it is aimed at preserving Baby B because Baby A isn’t likely to survive. Only if it appears that Baby A will not survive would we consider surgical options of FLP or Cord Occlusion. FLP is still a choice until the vessels become too large or if my placenta is too complicated to allow FLP. Which would leave us with cord Cord Occlusion: to be clear this laser sealing of Joshua’s umbilical cord along with lethal injection – it’s choosing to humanely end our baby’s life in the hope we can save Daniel.
These words below are so sterile and clinical but they mean choosing a car seat and a casket, or two caskets. In real life, these words are heart rending to the woman carrying these babies, seeing them on ultrasound with all of their fingers and toes, ears and lips, fully formed, approx. 10 inches long, occasionally sucking their thumbs or touching each other. They are my babies and I want to hold them, see them grow, hear them giggle, kiss their owies and hear them say “all better.” As a mom, I must hold the reality of losing them in one hand and the reality of their survival in the other every day and somehow remain sane in the duality.
Review of sIUGR Type 3
Unpredictable pattern of intermittent blood flow in the umbilical artery of the growth-restricted twin (forward, absent or reversal). In other words, only occasionally is the blood flow in the artery absent or flowing in a reverse direction. This type of blood-flow pattern is unique to monochorionic twins with sIUGR. It occurs when large arterio-arterial connections are present, allowing shared blood to flow back and forth between the twins.
Average age at delivery is 30 weeks gestation
In up to 15 percent of cases, the growth-restricted twin may not survive, which can also impact the neurodevelopment of the normally growing twin.
Whether or not the condition will change or worsen during pregnancy is difficult to predict from the ultrasound images. Babies with type 3 sIUGR are born, on average, during the 30th to 32nd week of pregnancy. Their overall survival rate is 80 percent.
Management of sIUGR may include continued observation with ultrasound surveillance or fetal therapy. Your recommended treatment will depend upon the type of sIUGR your twins are diagnosed with.
Treatment options for sIUGR
Expectant management: This involves continued close ultrasound surveillance throughout the pregnancy. We currently recommend expectant management for most Type 1 sIUGR and dichorionic twins.
Selective cord occlusion: This procedure may be offered if you have monochorionic twins with Type 2 or Type 3 sIUGR. Selective cord occlusion is a minimally invasive procedure that stops blood flow to the growth-restricted twin. The goal is to optimize the outcome for the normally growing twin. The procedure can be performed using bipolar cord coagulation, interstitial laser, or microwave ablation.
Fetoscopic laser photocoagulation: In select cases this minimally invasive surgery can be used to laser ablate (seal) blood vessels that are shared between the babies. Similar to selective cord occlusion, the goal of therapy is to optimize the outcome for the normally growing twin. Delivery: If sIUGR is discovered later in the pregnancy or the condition progresses after the pregnancy reaches its 24th to 26th week, delivery of the babies may be the best option. How is selective intrauterine growth restriction (sIUGR) treated after birth? Most babies with sIUGR are born prematurely, but our goal will be to prolong your pregnancy for as long as possible.
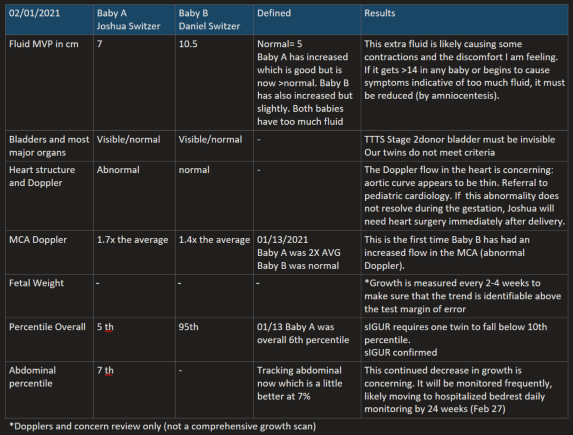
Today’s ultrasound and Doppler studies now indicate that the TTTS is not the major threat anymore. Baby A’s fluid MVP has increased to over 4 Baby B’s has increases slighty nearing 10 (we’re told at >14 the pressure will begin to cause health issues in Baby B. Having said that, right now Baby B is in the 98th percentile: he’s a giant due to all the blood flow he is getting. Baby A is in the 10th percentile for growth. The babies have a 25% size difference which is normal but indicating growth restriction. If Baby A falls below the 10th percentile, the diagnosis will be Selective Intrauterine Growth Restriction (sIUGR) which is similar to TTTS but appears to be even less treatable.
What is selective intrauterine growth restriction?
Monochorionic twins are twins that share a single placenta. Selective intrauterine growth restriction (sIUGR) occurs when there is unequal placental sharing which leads to suboptimal growth of one twin. In cases of sIUGR, the estimated fetal weight of the smaller, growth-restricted twin usually falls below the 10th percentile. This will usually result in more than a 25 percent weight difference between the twins.
sIUGR is estimated to occur in approximately 10 percent of monochorionic twin pregnancies. There are three types of sIUGR that are determined by the blood flow pattern in the umbilical artery of the growth-restricted twin.
The Fetal Health Foundation explains that severe cases of monochorionic twins with SIUGR show ultrasound evidence of abnormal blood flow through the umbilical artery of the poorly grown twin. In this circumstance, spontaneous death of this baby within the womb may occur in up to 40% of cases. Because of the blood vessels that link the twin’s circulatory system together, death of one twin may result in severe drop in blood pressure of the other twin and subsequent brain damage (up to 30%) or death (up to 40%). This complication results from the hemorrhage of blood from the appropriately grown twin into the demised SIUGR twin.Because the adverse effects to the appropriately grown twin is mediated through the blood vessels that link the circulations of the twins, it has been suggested that obliteration of these vascular communications may result in improved outcomes for the normally grown twin. Separation of the circulations may be done using the surgical techniques which were originally developed for the treatment of twin-twin transfusion syndrome. (Selective Intrauterine Growth Restriction (SIUGR) – Facts – Fetal Health Foundation)
Causes
The principle cause for the development of sIUGR in monochorionic twins is unequal placental sharing. The growth-restricted twin has a smaller share of the placenta, which over time results in abnormal blood flow and less growth. This could lead to death of the growth-restricted twin. Because the shared placenta also contains shared blood vessels between the twins (vascular communications), sIUGR also impacts the development of the brain and nervous system in the normal twin (neurodevelopment).
Symptoms
There are no physical symptoms of sIUGR that you, as a mother, would feel. sIUGR is a diagnosis made exclusively through ultrasound examination.
Evaluation and diagnosis
Accurate diagnosis is extremely important in distinguishing sIUGR from other diagnoses such as twin-twin transfusion syndrome (TTTS). TTTS and sIUGR both involve a shared placenta, but are differentiated by the type of vascular connections between the twins.
These differences can be very subtle. In TTTS, there is a very characteristic and progressive series of changes that happens to each twin. In sIUGR, the distribution of blood is more balanced, but because the growth-restricted twin has a much smaller portion of the placenta, the resistance in the umbilical artery is much higher than normal, resulting in suboptimal fetal growth.
Types of sIUGR
sIUGR has been classified into three types based on specific blood flow patterns in the umbilical artery of the growth-restricted twin.
Type 1
Consistent forward flow in the umbilical artery of the growth-restricted twin
Average age at delivery is 34-35 weeks gestation
In most cases of type 1 sIUGR, the babies’ condition remains stable throughout the pregnancy, although in up to 15 percent of cases, the sIUGR progresses as the pregnancy continues.
The overall survival rate for babies with type 1 sIUGR is greater than 90 percent.
Type 2
Either persistent absent blood flow or persistent reversal of blood flow in the umbilical artery of the growth-restricted twin
Average age at delivery is 26-32 weeks gestation
Babies with type 2 sIUGR have a guarded prognosis.
About 90 percent of cases worsen as the pregnancy continues.
Extreme preterm delivery is common among babies with type 2 sIUGR, often before the 30th week of pregnancy.
Type 3
Unpredictable pattern of intermittent blood flow in the umbilical artery of the growth-restricted twin (forward, absent or reversal). In other words, only occasionally is the blood flow in the artery absent or flowing in a reverse direction. This type of blood-flow pattern is unique to monochorionic twins with sIUGR. It occurs when large arterio-arterial connections are present, allowing shared blood to flow back and forth between the twins.
Average age at delivery is 30 weeks gestation
In up to 15 percent of cases, the growth-restricted twin may not survive, which can also impact the neurodevelopment of the normally growing twin.
Whether or not the condition will change or worsen during pregnancy is difficult to predict from the ultrasound images. Babies with type 3 sIUGR are born, on average, during the 30th to 32nd week of pregnancy. Their overall survival rate is 80 percent.
Treatment
Management of sIUGR may include continued observation with ultrasound surveillance or fetal therapy. Your recommended treatment will depend upon the type of sIUGR your twins are diagnosed with.
Treatment options include the following:
Expectant management: This involves continued close ultrasound surveillance throughout the pregnancy. We currently recommend expectant management for most Type 1 sIUGR and dichorionic twins.
Selective cord occlusion: This procedure may be offered if you have monochorionic twins with Type 2 or Type 3 sIUGR. Selective cord occlusion is a minimally invasive procedure that stops blood flow to the growth-restricted twin. The goal is to optimize the outcome for the normally growing twin. The procedure can be performed using bipolar cord coagulation, interstitial laser, or microwave ablation.
Fetoscopic laser photocoagulation: In select cases this minimally invasive surgery can be used to laser ablate (seal) blood vessels that are shared between the babies. Similar to selective cord occlusion, the goal of therapy is to optimize the outcome for the normally growing twin.
Delivery: If sIUGR is discovered later in the pregnancy or the condition progresses after the pregnancy reaches its 24th to 26th week, delivery of the babies may be the best option. How is selective intrauterine growth restriction (sIUGR) treated after birth? Most babies with sIUGR are born prematurely, but our goal will be to prolong your pregnancy for as long as possible.
We recommend that your babies are born at a hospital able to care for premature babies.
Treatment for Type 1 sIUGR
You will undergo continued weekly observation with your local maternal-fetal medicine specialist. Weekly or twice weekly ultrasounds closely monitor the growth of both twins and watch for progression to Type 2 or Type 3 sIUGR which may indicate prompt referral for fetal therapy.
Because preterm deliveries are common in pregnancies affected by sIUGR, consultation with neonatology and a specialized delivery center can help you plan for this possibility.
Treatment for Type 2 and Type 3 sIUGR
Along with weekly observation by your maternal-fetal medicine specialist, we may recommend fetal therapy in the form of selective cord occlusion.
Selective cord occlusion is a minimally invasive surgical procedure that seeks to improve the outcome for the normally growing twin by stopping the blood flow to the growth-restricted twin in a way that minimizes impact the neurodevelopment and survival of the normally growing twin. Selective cord occlusion can be performed using bipolar cord coagulation (BCC) or radiofrequency ablation (RFA) procedures.