


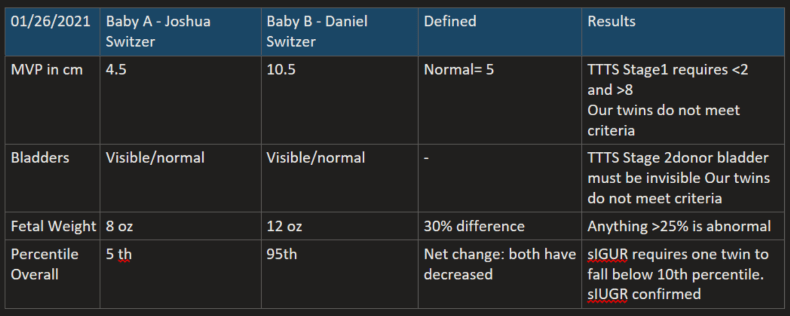
With normalized Dopplers, this week the TAPS diagnosis is put on the back burner along with TTTS. However, sIUGR is confirmed because Baby A’s growth falls below the 10th percentile, the diagnosis of Selective Intrauterine Growth Restriction (sIUGR) is confirmed. While sIUGR and our babies have Type 3.
Our treatment path is currently Expectant Management. As we do weekly or more frequent monitoring, conditions may change. Because the artery to artery flows between the babies are likely keeping Baby A alive, we will not consider surgery, because it is aimed at preserving Baby B because Baby A isn’t likely to survive. Only if it appears that Baby A will not survive would we consider surgical options of FLP or Cord Occlusion. FLP is still a choice until the vessels become too large or if my placenta is too complicated to allow FLP. Which would leave us with cord Cord Occlusion: to be clear this laser sealing of Joshua’s umbilical cord along with lethal injection – it’s choosing to humanely end our baby’s life in the hope we can save Daniel.
These words below are so sterile and clinical but they mean choosing a car seat and a casket, or two caskets. In real life, these words are heart rending to the woman carrying these babies, seeing them on ultrasound with all of their fingers and toes, ears and lips, fully formed, approx. 10 inches long, occasionally sucking their thumbs or touching each other. They are my babies and I want to hold them, see them grow, hear them giggle, kiss their owies and hear them say “all better.” As a mom, I must hold the reality of losing them in one hand and the reality of their survival in the other every day and somehow remain sane in the duality.
Review of sIUGR Type 3
- Unpredictable pattern of intermittent blood flow in the umbilical artery of the growth-restricted twin (forward, absent or reversal). In other words, only occasionally is the blood flow in the artery absent or flowing in a reverse direction. This type of blood-flow pattern is unique to monochorionic twins with sIUGR. It occurs when large arterio-arterial connections are present, allowing shared blood to flow back and forth between the twins.
- Average age at delivery is 30 weeks gestation
- In up to 15 percent of cases, the growth-restricted twin may not survive, which can also impact the neurodevelopment of the normally growing twin.
- Whether or not the condition will change or worsen during pregnancy is difficult to predict from the ultrasound images. Babies with type 3 sIUGR are born, on average, during the 30th to 32nd week of pregnancy. Their overall survival rate is 80 percent.
Management of sIUGR may include continued observation with ultrasound surveillance or fetal therapy. Your recommended treatment will depend upon the type of sIUGR your twins are diagnosed with.
Treatment options for sIUGR
Expectant management: This involves continued close ultrasound surveillance throughout the pregnancy. We currently recommend expectant management for most Type 1 sIUGR and dichorionic twins.
Selective cord occlusion: This procedure may be offered if you have monochorionic twins with Type 2 or Type 3 sIUGR. Selective cord occlusion is a minimally invasive procedure that stops blood flow to the growth-restricted twin. The goal is to optimize the outcome for the normally growing twin. The procedure can be performed using bipolar cord coagulation, interstitial laser, or microwave ablation.
Fetoscopic laser photocoagulation: In select cases this minimally invasive surgery can be used to laser ablate (seal) blood vessels that are shared between the babies. Similar to selective cord occlusion, the goal of therapy is to optimize the outcome for the normally growing twin.
Delivery: If sIUGR is discovered later in the pregnancy or the condition progresses after the pregnancy reaches its 24th to 26th week, delivery of the babies may be the best option.
How is selective intrauterine growth restriction (sIUGR) treated after birth?
Most babies with sIUGR are born prematurely, but our goal will be to prolong your pregnancy for as long as possible.
